It’s all about perspective.
And tenacity.
And determination.
And character.
 After NASA Astronaut Scott Kelly and Russian cosmonaut Mikhail Kornienko of Roscosmos got home from a year in space this past spring, the US Congress began examining whether to provide lifetime health benefits to astronauts. Many are ex-military and get benefits that way. NASA will monitor recipients for long-duration mission health planning.
After NASA Astronaut Scott Kelly and Russian cosmonaut Mikhail Kornienko of Roscosmos got home from a year in space this past spring, the US Congress began examining whether to provide lifetime health benefits to astronauts. Many are ex-military and get benefits that way. NASA will monitor recipients for long-duration mission health planning.
At industrial design school, one of my human factors projects was a spider-like astrogeology exoskeleton, designed so geologists could move along a cliff face looking at strata. And the thinking fed into iteration #1 of my design thesis: one of the first social web wearables; a performance tool for whitewater slalom athletes. But a bigger aspect of the thinking keeps coming back to me: A question that might help address the dilemma of bone loss. A question that keeps coming back after doing WarriorHealth CombatCare and finding out about the fine work done at Walter Reed National Military Medical Center in Bethseda, MD.
 Is a veteran with paraplegia or no legs the natural spacecraft driver?
Is a veteran with paraplegia or no legs the natural spacecraft driver?
Since bone density loss is a key barrier to long-term low gravity living…aren’t technically-trained veteran paraplegians and double amputees great candidates for the astronaut corps? Does a fighter pilot have the discipline, skill and temperament to be a launch driver? Does an armored division tanker have the skills to be an in-flight systems specialist?
Does USMC Corporal Todd Love (an incredibly inspirational guy! seen here) really need legs to operate in micro-gravity, when he might only need wheels on the ground? (As you can see, he does not need legs whatsoever).
I ask you…
Could this approach create uplifting new opportunities to serve and thrive in a way that makes the unavoidable SCI injury extraordinarily valuable?
Aren’t two-legged people naturally less abled in the spaceflight environment?
Who is the more-natural space-athlete?
Who is the more-natural astronaut?
David Huer
Numbers
US veterans with Spinal Cord Injury (SCI) as of 2008: 26,000 veterans
http://www.military.com/benefits/veterans-health-care/veterans-with-spinal-cord-injury-disorders.html
US citizens with SCI: 240,000 and 337,000 people
New injuries per year, as of 2015: 12,500 people
http://www.sci-info-pages.com/facts.html
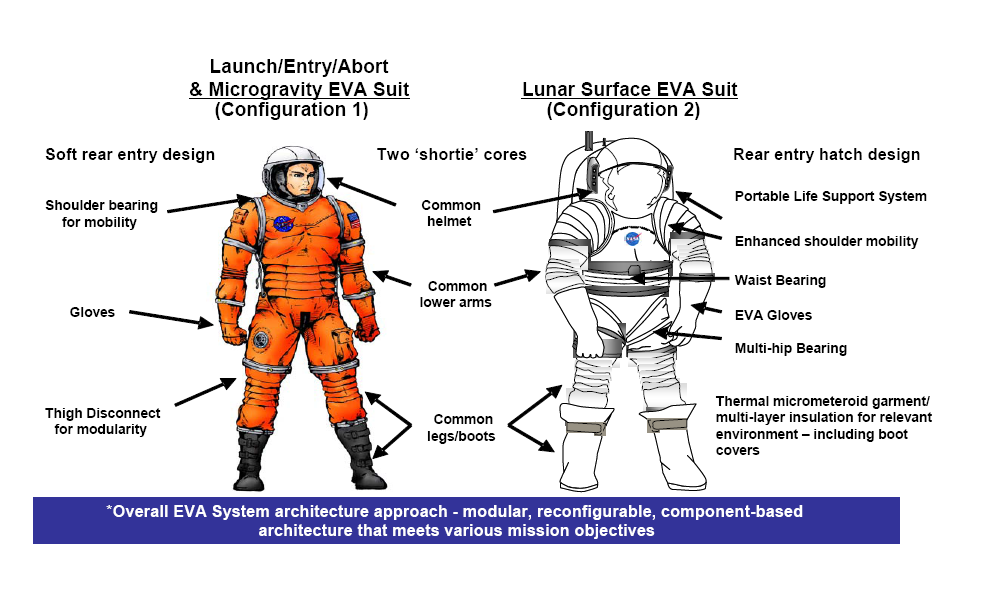
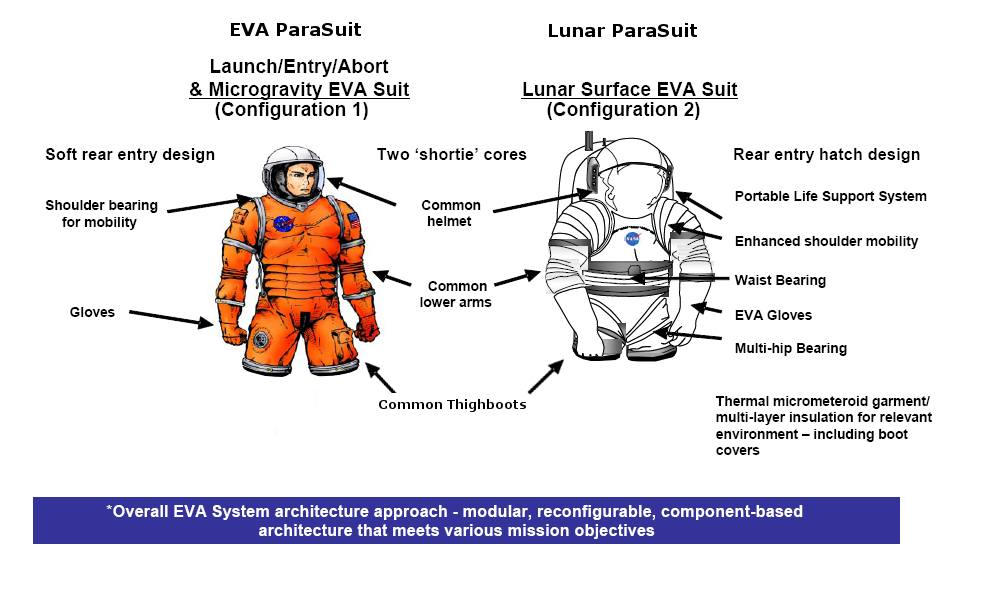
Latest EVA suit made by Oceaneering Inc. (Houston, TX):
http://www.nasa.gov/pdf/246726main_ConstellationSpaceSuitSystemBriefing.pdf
Interesting aspects of design/safety aspects
* Effect to bone mass/density and to body functions
* Pant legs + boots: removed – aperture and material needs cut by ~40%, with 5 apertures (head, left & right arm, left & right leg) reduced to 3.
* Electronic components & new designs for torso & new “thighboots”
* “Thighboots” reduce the dangers of entanglement & provide push-off tasking as needed
* External prosthetics designed to attach to thighboots
Healthcare research outcome:
Could NASA, the VA and DoD assess impact on SCI to help society groundside?
Images:
US Astronaut Tom Jones (STS-129): https://skywalking1.files.wordpress.com/2009/11/tom-reaching-for-lab-umbilicals-sts098-330-0071.jpg
USMC Corporal Todd Love and Team X-T.R.E.M.E. competing in The Spartan Race, Leesburg, VA, 2012: http://www.dailymail.co.uk/news/article-2195897/Triple-amputee-veteran-completes-grueling-10-5-mile-endurance-race-called-The-Beast-hours-honor-fallen-U-S-soldiers.html
Constellation EVA Spacesuit: NASA http://www.nasa.gov/pdf/246726main_ConstellationSpaceSuitSystemBriefing.pdf
(Image modified with removal of lower extremities in image)

 The UK and its federated daughter states – former colonies such as Australia and Canada – may not be much different. Canada is a collection of independent provinces, each with its own powers, conjoined as a federation for shared purpose.
The UK and its federated daughter states – former colonies such as Australia and Canada – may not be much different. Canada is a collection of independent provinces, each with its own powers, conjoined as a federation for shared purpose.